Whole-Person Care as the Foundation of Modern Home-Based Visits

Part 1 in a series on whole-person CHAs
In today’s risk environment, a home-based Comprehensive Health Assessment (CHA) is often the most meaningful clinical touchpoint a health plan has with its most complex members. For some, it is the only clinical interaction they will have all year. The question is no longer whether to conduct CHAs. It is whether those assessments are designed to meaningfully change outcomes.
In this post, we examine whole-person care as the organizing principle behind a high-performing home-based care model. We explore what the philosophy means in practice, how Matrix embeds it into care delivery, and why it directly influences outcomes for members and performance for health plans.
What whole-person care means in the context of home-based care
At its core, the whole-person care approach reflects the reality that a member’s health cannot be understood through clinical data alone. Medical conditions, daily environment, functional limitations, social supports and enrollee benefit design all interact. Addressing them in isolation often leaves meaningful care gaps unaddressed.
In the home, these dimensions are not abstract. They are visible, contextual and actionable. Whole-person care changes how a clinician interprets what they observe in the home. A blood pressure reading is not just a number, instead it may reflect medication confusion, caregiver strain or transportation barriers preventing follow-up care. A mobility limitation may signal fall risk, untreated pain or environmental hazards. By assessing clinical findings alongside environmental, behavioral and social factors in real time, the CHA becomes a more accurate reflection of a member’s true health status. It also provides a consistent lens across patient populations, markets and benefit structures, ensuring that care decisions remain grounded in real-world context rather than fragmented data points.
Too often, in-home assessments become checklist-driven documentation exercises. They capture diagnoses but fail to translate insight into coordinated action. When findings do not drive follow-through, the opportunity is lost. Whole-person care ensures the visit is not isolated from the rest of the care ecosystem. It aligns the member, the primary care provider and the health plan around actionable next steps. That reality often becomes clear in small, unexpected moments during a visit.
Three interlocking components of whole-person care
Whole-person care is not a discrete service or add-on. It is a care model that underpins how home-based care is delivered overall. Anchoring the concept in real-world application helps illustrate how it translates into practice. Matrix operationalizes whole-person care through three core interlocking components.
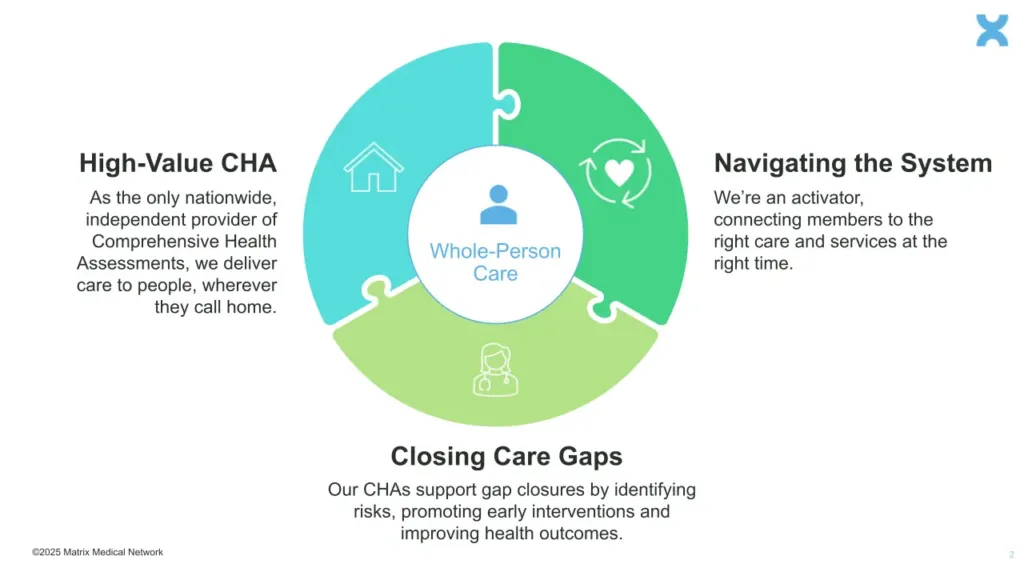
- High-value CHAs
- High-value CHAs pair comprehensive clinical evaluation with curated, in-the-moment patient education and clear next steps. Matrix clinicians don’t just document conditions; they help members understand medications, follow-up needs and preventive care priorities during the visit. Just as importantly, they feed critical, actionable information back to the health plan and the member’s primary care provider, surfacing risks and barriers that would otherwise remain hidden and enabling earlier intervention and better coordination. For health plans operating in value-based models, this improves not only member care but also risk accuracy, quality performance and total cost of care.
- Closing care gaps before they escalate
- Closing care gaps centers on identifying risks through in-home screenings and proactive assessment and acting before those risks escalate. During the CHA, clinicians conduct clinical and preventive screenings that may not occur consistently in traditional settings, including evaluations for unmanaged chronic conditions, fall risk, cognitive decline, medication adherence and behavioral health needs. By detecting these gaps in real time and reinforcing timely follow-up, the visit helps prevent avoidable deterioration and supports better outcomes over time.
- Navigating the system to ensure follow-through
- Navigating the system focuses on ensuring that what is identified during the visit translates into meaningful follow-through. When clinical risks, care gaps or unmet needs are uncovered, Matrix clinicians connect members to the appropriate next step, whether that means communicating findings to the primary care provider, initiating a care management referral or coordinating with health plan teams and community-based services to support stabilization. The goal is not simply to surface issues, but to ensure continuity by aligning the member, the PCP and the plan around clear, actionable next steps that advance health and wellness beyond the home visit.
Together, these three components create a consistent structure for delivering whole-person care during home-based encounters.
Why acting on the whole-person care philosophy is urgent
For risk-bearing providers and payers, ensuring that home-based services have whole-person care at their center is not a nice-to-have—it is an imperative that cannot wait.
The urgency stems from two factors.
- First, even patients who are receiving regular in-office visits may have risk factors that will go undetected without eyes on their home environment.
- Second, every year, some plan members are not receiving regular in-office visits. Instead, they are becoming disconnected from, and invisible to, the healthcare system. As explored in a prior post on the “unseen five percent,” for a surprisingly large share of patients, the CHA is the most meaningful (and sometimes only) clinical interaction the patient has for a 12-month period.
These factors raise the stakes for ensuring that CHAs are not simply done but done well.
Unaddressed risks, barriers and clinical/social needs have significant consequences for individual patients, families and plan success as a whole. There is a growing body of evidence that links unaddressed behavioral health needs and social isolation to avoidable hospital utilization and poorer chronic disease management. In a meta-analysis of 41 randomized studies, psychosocial and social-support interventions were associated with roughly 25% lower odds of healthcare use overall, including a 36% reduction in emergency care visits. Randomized trials of community-based care navigation have likewise shown strong impact, with one study finding participants were 56% less likely to be readmitted within 30 days. When social and functional barriers are identified and addressed early, avoidable utilization often follows.
For healthcare organizations investing in home-based care, the question is not whether to conduct CHAs — it is whether those assessments are designed to meaningfully change the trajectory of a member’s health. When grounded in whole-person care, an in-home assessment program can surface hidden risks, reinforce education, close care gaps and translate insight into coordinated action across the care ecosystem. When assessments do not drive coordinated follow-through, the opportunity to alter outcomes is lost. When they do, the CHA becomes a catalyst for better member engagement, stronger care coordination and improved plan performance.
What’s next
Whole-person care is not a philosophical overlay. It is the operational foundation that determines whether a home visit meaningfully alters a member’s health trajectory and whether it improves plan performance.
A CHA program that does not translate insight into coordinated action will not change outcomes. On the other hand, one that does can reshape how members engage with the healthcare system and how plans manage risk across their population.
In Part 2, we’ll explore in greater detail what clinical staff members at Matrix do during the CHA itself, showcasing concrete, visit-level examples that illustrate how care delivery and patient experience change when whole-person care is executed well.
Related Posts
Nutrition as a Vital Sign: Addressing the Hidden SDOH Barrier
Nutrition is more than a lifestyle choice; for high-risk members, it is a clinical prerequisite for successful chronic disease management. While many risk-bearing organizations acknowledge the impact of Social Determinants of Health (SDOH), food insecurity often remains a “hidden” barrier that traditional office-based screenings fail to…
What Medicaid Funding Changes Mean for At-Risk Patients
The Medicaid landscape is undergoing its most significant structural transformation since the expansion era of the last decade. As the fiscal protections of the pandemic era recede, health plans and state agencies are confronting a convergence of federal funding shifts, changing member demographics and a more rigorous regulatory environment. For…
How Telehealth Policy Shifts Affect Home-Based Care Delivery
The American care delivery system has reached a critical inflection point in 2026. As we transition from pandemic-era emergency measures toward a permanent regulatory infrastructure, risk-bearing organizations face a strategic adjustment: reconciling the convenience of digital health with new federal mandates for physical clinical touchpoints. The overarching theme of 2026…